Epidemiology and Demographics of SSB Consumption (Global & India Focus)
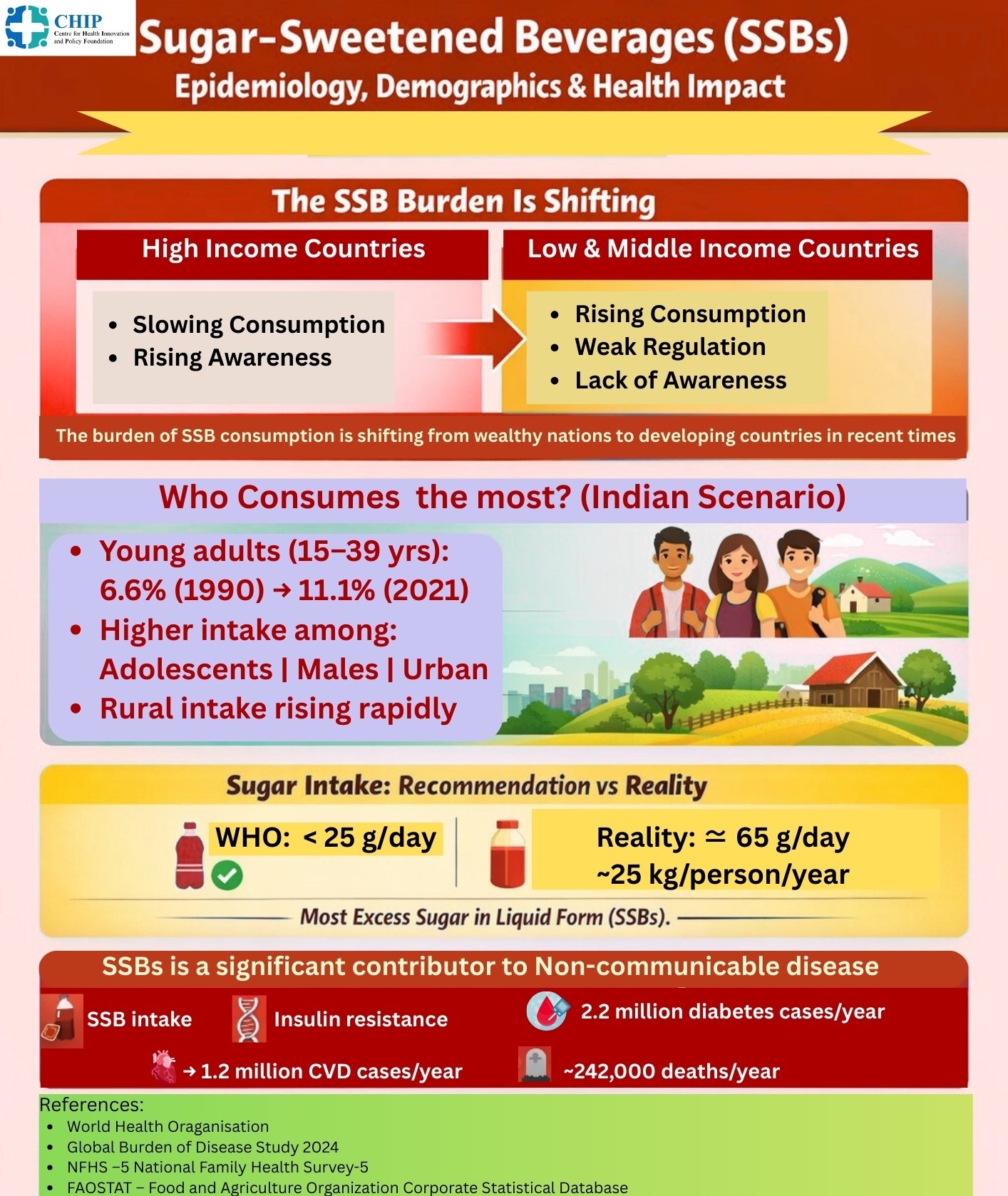
The burden of SSB consumption has shifted from high-income countries to LMICs, particularly in the Global South, where it is now a major driver of NCDs(1). While fiscal policies have slowed intake in some high-income settings, multinational beverage companies continue to expand aggressively into emerging markets. Globally, the prevalence of high SSB intake among young adults (15–39 years) increased from 6.6% in 1990 to over 11.1% in 20212. SSB consumption contributes to approximately 2.2 million new cases of type 2 diabetes and 1.2 million cardiovascular disease cases annually, with attributable deaths increasing from about 150,000 in 1990 to over 240,000 in the 2020s (3,4,5). FAOSTAT data indicate that global per-capita sugar availability (~65 g/day) far exceeds the WHO-recommended limit of <25 g/day (4,5). India exemplifies this rapid nutrition transition. NFHS-5 and allied national data show increasing displacement of traditional diets by ultra-processed foods and SSBs(6). About 22.4% of men and 0.7% of women aged 15–49 report alcohol drink consumption, with higher intake among adolescents, males, and urban populations, though rural consumption is rising through affordable small-pack sales(7,8). Overweight and obesity among Indian men increased by 146% between NFHS-3 and NFHS-5, while retail sales of ultra-processed foods and beverages grew at a CAGR of 13.7% between 2011 and 2021, reaching USD 37.9 billion(9). Average sugar intake in India is estimated at ~25 kg/person/year, far exceeding WHO recommendations, with higher income and literacy initially correlating with increased consumption (10,11).
Health Impacts of Sugar-Sweetened Beverages
1. Excess Energy Intake, Weight Gain, and Obesity
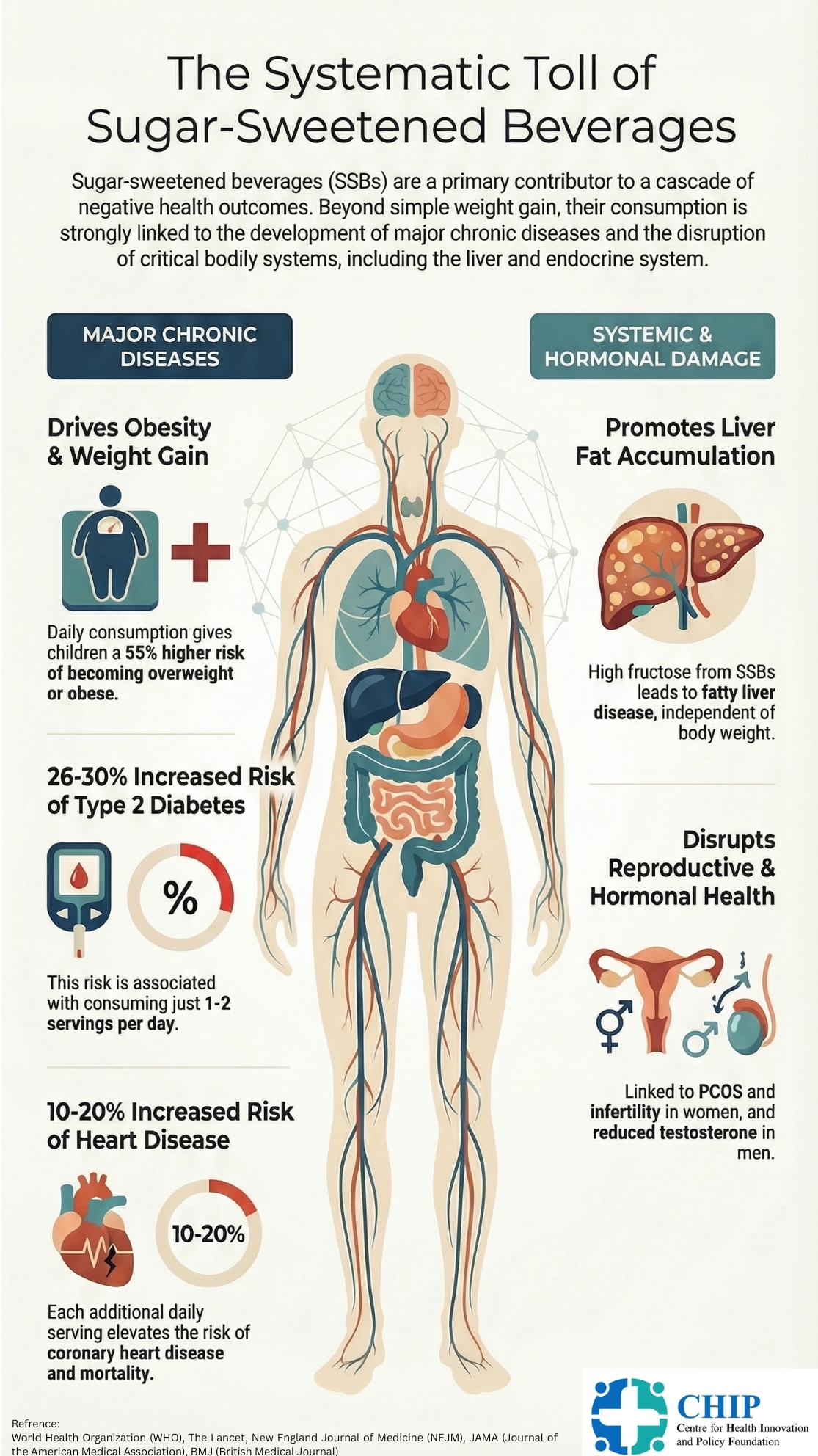
SSBs provide large amounts of rapidly absorbable sugars with minimal satiety, leading to excess energy intake and weight gain. Each additional daily serving is associated with approximately 0.45 kg greater weight gain over four years in adults, while children consuming ≥1 SSB/day have a 55% higher risk of overweight or obesity (12). WHO concludes that reducing SSB intake lowers population-level obesity risk (13).
2. Type 2 Diabetes Mellitus
Habitual SSB consumption is strongly associated with type 2 diabetes, even after adjustment for body mass index, suggesting mechanisms beyond adiposity. Intake of 1–2 servings/day increases diabetes risk by 26–30%, with a substantial proportion of global diabetes incidence attributable to SSBs (14,15).
3. Cardiovascular Disease
SSB intake is linked to coronary heart disease, stroke, and cardiometabolic mortality through mechanisms including insulin resistance, dyslipidaemia, endothelial dysfunction, and inflammation. Each additional daily serving increases coronary heart disease risk by 10–20% and is associated with higher cardiovascular and all-cause mortality(15,16).
4. Liver Disease and MAFLD
SSBs are a major source of dietary fructose, promoting hepatic fat accumulation, insulin resistance, and inflammation (17,18). In postmenopausal women, daily sugar-sweetened beverage consumption (≥1 serving/day) was associated with an approximately 85% higher risk of hepatocellular carcinoma and a 68% higher risk of chronic liver disease mortality, compared with low intake (19). Fructose-induced hepatic fat accumulation occurs independent of body weight and contributes to metabolic dysfunction–associated fatty liver disease (MAFLD), which is closely linked to cardiovascular mortality (18,20,21,22).
5. Sexual Hormones and Reproductive Health
SSB-induced insulin resistance and adiposity disrupt endocrine homeostasis. Chronic hyperinsulinemia suppresses hepatic sex hormone–binding globulin (SHBG), increasing free sex hormone levels and cardiometabolic risk(20). In women, high SSB intake contributes to hyperandrogenism, polycystic ovary syndrome (PCOS), menstrual irregularities, and infertility, making sugar reduction central to PCOS management(23). In men, excess sugar intake is associated with visceral adiposity, reduced testosterone, infertility, sarcopenia, and adverse cardiometabolic outcomes (24).
Taxation on Sugar-Sweetened Beverages in India
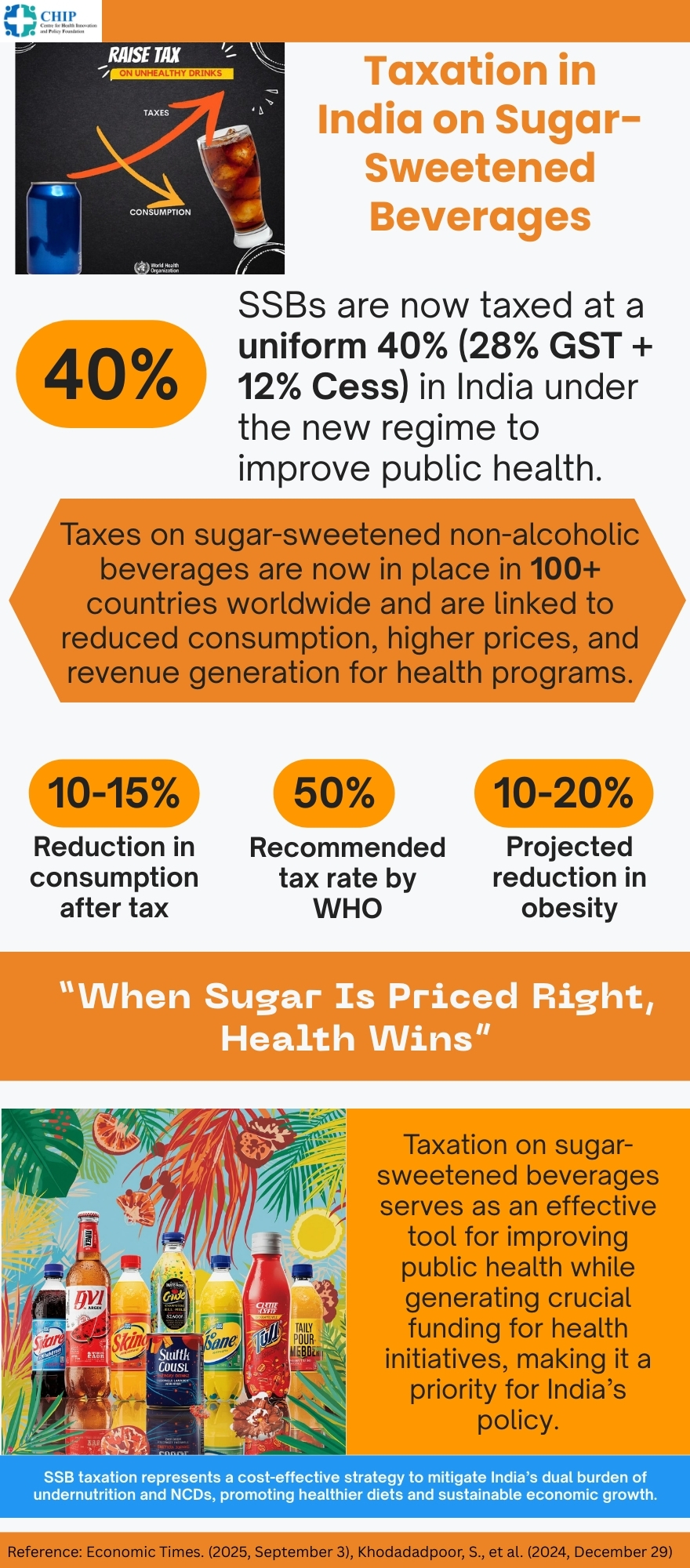
SSBs classified under HSN code 2202 are subject to taxation under India’s GST framework (25). Following the 56th GST Council meeting in September 2025, SSBs were placed under a “sin tax” category, with a uniform 40% GST rate applied to aerated and sugar-sweetened beverages (26-29). This replaced the earlier structure of 28% GST plus a 12% compensation cess, maintaining an effective deterrent rate while simplifying taxation(25,27). The policy aligns with WHO recommendations advocating 20–50% taxation to reduce consumption and generate revenue for health programs (30,31). Health Burden and Economic Rationale Globally, over 50 countries have implemented SSB taxes, achieving average consumption reductions of 10–15% (31) Modeling studies suggest that increasing India’s tax to 50% and earmarking revenues for health and nutrition programs could further enhance public health impact (30–32). From a health economics perspective, SSB taxation functions as a Pigovian tax, correcting externalities linked to healthcare costs and productivity losses from obesity and diabetes (30,33). India’s current 40% GST is projected to reduce consumption by 10–20%, avert future NCD cases, and generate fiscal space for public health investment (33,34,35).

Labelling of SSBs
Food labelling in India is regulated by the Food Safety and Standards Authority of India (FSSAI) under the Food Safety and Standards Act, 2006(36). Mandatory labelling includes nutritional information, ingredient lists, and declaration of added sugars, though no specific warning labels for high sugar content are currently required. Evidence shows that health warnings significantly reduce SSB purchase intentions and consumption, particularly among children (37,38). While several jurisdictions in the USA have proposed warning labels, only San Francisco has implemented them(39).
In September 2022, FSSAI issued draft amendments proposing Front-of-Pack Nutrition Labelling (FOPNL), identification of High Fat, Sugar, and Salt (HFSS) foods, disclosure of key ingredient percentages, dietary fiber content, and introduction of the Indian Nutrition Rating (INR) system(40). The INR assigns star ratings from 0 (least healthy) to 5 (healthiest), enabling consumers to make informed choices.